 |
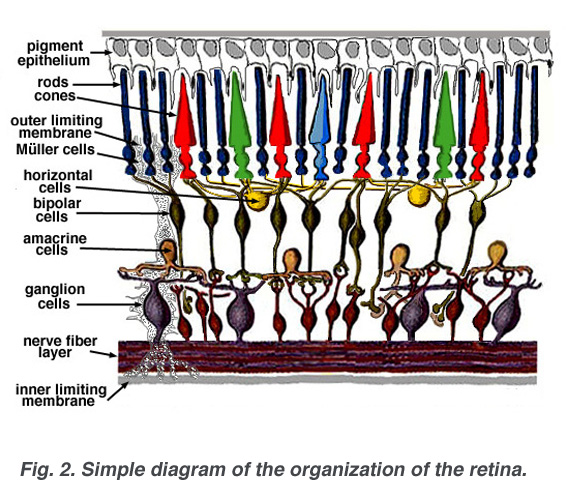
| Figure Reference: Med.Utah.edu (linked, pl click) |
The Electroretinogram: Clinical Applications by Donnell J. CreelIn general, intraopertive neurophysiological monitoring teams do not conduct ERG or EOG in the Operating room set up, it is rather cumbersome and difficult to get a reliable readings combined with the difficulty of placing the recording electrode and risks that are associated with the procedure. However, Donnell in its Chapter on"The electroretinogram" presents the latest developments that record the status of retinal function using skin electrodes and he also sheds light on the recent advancement in ERG the multifocal retiongram. Whether you are going to conduct this test or not, if you are interested in all the evoked potentials and the basics, this is an excellent reading material. Enjoy.
Electrophysiological testing of patients with retinal disease began in clinical departments in the late nineteen forties. Under the influence of the Swedish pioneers, Holmgren (1865) and Granit (1933), the electroretinogram was being dissected into component parts and early intraretinal electrode studies were beginning to tell which cells or cell layers gave rise to the various components. A detailed discussion of the electroretinogram, or ERG as it is commonly abbreviated, is found in the accompanying chapter by Ido Perlman. A little after the introduction of the ERG as a test of the state of the patient’s retina, another diagnostic test called the electrooculogram (EOG) was introduced to the clinic (Arden et al., 1962). The EOG had advantages over the ERG in that electrodes did not touch the surface of the eye. The changes in the standing potential across the eyeball were recorded by skin electrodes during simple eye movements and after exposure to periods of light and dark. Over the years ERG recording techniques have become progressively more sophisticated in the clinical setting. With the advent of perimetry, optical coherence tomography (OCT) and pattern ERG techniques, more precise mapping of dysfunctional areas of the retina is now possible. The most recent advance in ERG technology is the multifocal electroretinogram (mfERG). The mfERG provides a detailed assessment of the health of the central retina.