Brain damage after eating KFC's contaminated chicken twister?, Ouch..! are you still going to KFC?. I have to say that it has been years since I even had a glimpse of the KFC building, let alone go inside to buy some meal, it is simply a disgusting food place, no wonder why the Australian court ordered KFC to pay $8Million to a 7 year old girl who suffered Salmonella infection after eating KFC food.
That is a one disgusting place to go for food?.
Friday, April 27, 2012
KFC Chicken Twister & Salmonella, watch out!

Thursday, March 15, 2012
Bis- Is it Reliable?, what do the Anesthesiologists & Surgeons must know about Bis?.
New England Journal of Medicine is one of the Most respected and trustable medical journals out there, personally I place NEJM on top of some of even the well known American medical journals without a slightest doubts.And, this time it is the NEJM that has published some important results on BIS monitor usage by anesthesiologists inside the Operating Rooms.. The question many of the medical professionals must raise about this little tool is, is it a valuable technique to be used about patient's awareness or sleep/awake status during surgical procedures??. Now we know for sure from this study that the actual "validity" of BIS is seriously flawed and questionable?, further lead to a massive Re-call of FDA approved Bis monitors by the manufacturer Covidien, "Covidien PLC (COV) unveiled an expanded recall of its BIS Bilateral sensors" (Wall Street Journal)
Here is the RESULT of a study published in NEJM:
RESULTS
A total of 7 of 2861 patients (0.24%) in the BIS group, as compared with 2 of 2852 (0.07%) in the ETAC group, who were interviewed postoperatively had definite intraoperative awareness (a difference of 0.17 percentage points; 95% confidence interval [CI], −0.03 to 0.38; P=0.98). Thus, the superiority of the BIS protocol was not demonstrated. A total of 19 cases of definite or possible intraoperative awareness (0.66%) occurred in the BIS group, as compared with 8 (0.28%) in the ETAC group (a difference of 0.38 percentage points; 95% CI, 0.03 to 0.74; P=0.99), with the superiority of the BIS protocol again not demonstrated. There was no difference between the groups with respect to the amount of anesthesia administered or the rate of major postoperative adverse outcomes.
This topic of whether or not BIS monitor can help the anesthesiologist regarding the level of anesthesiology administered to patient is enough, or deep enough for a surgical incision to be performed by surgeon without perturbing patient memory was under debate among professionals for quite sometime, but this research group headed by Michael S Avidan, the principle investigator along with a big team at Washington University School of Medicine clarified to a some extent and proves the major consensus in the field that bis is unreliable?, the patients may be sleep but not to an extent intended or needed by anesthesiologist, so the patient might still be able to recall some of the ongoing conversations or sounds in the OR, huh?.
It is not just about remembering what is going on in the OR while sleeping on the surgical bed, but beyond that the Pain the patient will be enduring and remembering the pain due to surgical procedure is simply unacceptable and need to be addressed by medical and health care communities immediately. As far as feeling or remembering the pain of a surgical knife cutting though lasts for few seconds to minutes, it still unacceptable medical practice for the patient to go through or endure such pain, we are not in a war zone or some third world where there is no proper medical facility or no other alternative but take a knife and cut in a emergency scenario?. However, what we are discussing here is about a totally equipped, highly advanced, ethically and medically justified planned surgical set up, and there is no execuse.
Here is the Link to the Full Study:
Study Evaluating Whether the Bispectral Index Prevents Patients at Higher Risk From Being Awake During Surgery and Anesthesia (BAG-RECALL)
First Received on May 16, 2008. Last Updated on January 3, 2011 History of Changes
| Sponsor: | Washington University School of Medicine |
|---|---|
| Collaborators: | Foundation for Anesthesia Education and Research American Society of Anesthesiologists University of Chicago University of Manitoba University of Michigan |
| Information provided by: | Washington University School of Medicine |
| ClinicalTrials.gov Identifier: | NCT00682825 |
Saturday, December 24, 2011
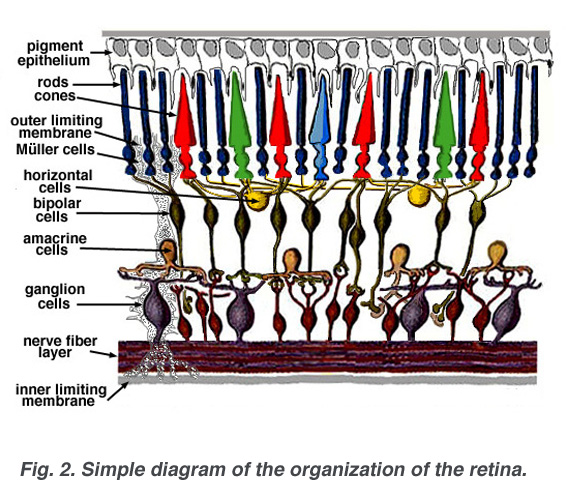
Electroretinogram by Donnell J Creel
 |
| Figure Reference: Med.Utah.edu (linked, pl click) |
The Electroretinogram: Clinical Applications by Donnell J. CreelIn general, intraopertive neurophysiological monitoring teams do not conduct ERG or EOG in the Operating room set up, it is rather cumbersome and difficult to get a reliable readings combined with the difficulty of placing the recording electrode and risks that are associated with the procedure. However, Donnell in its Chapter on"The electroretinogram" presents the latest developments that record the status of retinal function using skin electrodes and he also sheds light on the recent advancement in ERG the multifocal retiongram. Whether you are going to conduct this test or not, if you are interested in all the evoked potentials and the basics, this is an excellent reading material. Enjoy.
Electrophysiological testing of patients with retinal disease began in clinical departments in the late nineteen forties. Under the influence of the Swedish pioneers, Holmgren (1865) and Granit (1933), the electroretinogram was being dissected into component parts and early intraretinal electrode studies were beginning to tell which cells or cell layers gave rise to the various components. A detailed discussion of the electroretinogram, or ERG as it is commonly abbreviated, is found in the accompanying chapter by Ido Perlman. A little after the introduction of the ERG as a test of the state of the patient’s retina, another diagnostic test called the electrooculogram (EOG) was introduced to the clinic (Arden et al., 1962). The EOG had advantages over the ERG in that electrodes did not touch the surface of the eye. The changes in the standing potential across the eyeball were recorded by skin electrodes during simple eye movements and after exposure to periods of light and dark. Over the years ERG recording techniques have become progressively more sophisticated in the clinical setting. With the advent of perimetry, optical coherence tomography (OCT) and pattern ERG techniques, more precise mapping of dysfunctional areas of the retina is now possible. The most recent advance in ERG technology is the multifocal electroretinogram (mfERG). The mfERG provides a detailed assessment of the health of the central retina.
Saturday, November 26, 2011
The Year in Neurology, 2011 Drug approvals and New treatments for Neurological disorders?
Medscape Article:
Andrew N. Wilner, MD writes about the recent developments in basic science and clinical medicine to treat some of the impending neurological diseases, including several FDA approval on new drugs, interesting article.
A Look Back: Introduction
2011 has been a very exciting year for neurologists and their patients. Advances in basic science and disciplined clinical trials have led to drug approvals for the prevention of stroke and treatment of epilepsy. In addition, at least 2 oral drugs for relapsing-remitting multiple sclerosis, BG-12 and teriflunomide, boast positive results from phase 3 trials and are poised for approval by the US Food and Drug Administration (FDA).In 2010, the FDA approved dabigatran, a thrombin inhibitor, for anticoagulation in patients with nonvalvular atrial fibrillation. In November 2011, the FDA approved rivaroxaban, a once-daily oral factor Xa inhibitor, for the same indication. Another factor Xa inhibitor, apixaban, recently demonstrated superior results to warfarin in preventing stroke or systemic embolism, with less bleeding and lower mortality, and may soon be approved as well.[1]
Full article at Medscape linked at the top.
Thursday, November 10, 2011
NeuroPhysiology Fed Research Funding declined Significantly?
Research Crossroads published the following chart for Neurophysiology funding, pretty bleak is the research fundings in our field?.
Both Neurophysiology funding and number of grants for research has been steeply declined since 2006 and it is probably at the 1994-6 levels, the lowest of funding provided to Neurophysiology research during these periods since 1992


Both Neurophysiology funding and number of grants for research has been steeply declined since 2006 and it is probably at the 1994-6 levels, the lowest of funding provided to Neurophysiology research during these periods since 1992

Funding History?
Charted historical Neurophysiology funding.
Monday, September 12, 2011
IONM background, literature, history and Updates...!
Check out the latest news or reports topic and my upcoming editorial of animal electricity....!!
You Tube Video & Anguish of a Lay man about NeuroMonitoring?
You Tube Video & Anguish of a Lay man about NeuroMonitoring?
Oh I wish there was someone from Neuromonitoring field had noticed the following random ranting of a lay man with quite an Anguish tone filled with incredible painful experience of being Stalked by some Remote stuff?, that this man decided to call it remote neuromonitring?, since no one helped this guy, his confusion continues as this posting,. So far and no one clarified online or offline to this man, I had to stretch from already busy blog writing to even answer unrelated rants of this kind, finally I had to do it myself to bring attention of this issue both to this lay man and to the Neuromonitoring professionals.Dear Mr, Guy?,
Let me respectfully assert you that you have no idea or knowledge about Neuromonitoring or Remote Neuromoitoring, I wish you had consulted someone who knows about this field before making this public video that talks unintelligibly about a Scientific and Clinical Surgery field known as Intraoperative Neurophysiological Monitoring or in general known as Neuromonitoring.
Monday, February 28, 2011
Do you Smell: This is the Special Issue of ACS Chemical Senses published at SFN!
 For those interested in sensory modalities and the recent developments especially on olfactory system, this topic might of great interest. A special issue on chemical senses published at the Society for neuroscience site.
For those interested in sensory modalities and the recent developments especially on olfactory system, this topic might of great interest. A special issue on chemical senses published at the Society for neuroscience site.One of the most extensive research work of mine explores the ability of central nervous pathway "olfactory tract" regeneration following experimentally induced transection (simulation of certain type of traumatic damage), the results have already been published in many reputed journals, a fascinating finding indicating though CNS has limited abilities to regenerate, central tracts like olfactory pathway has enormous regenerative potentials even at the synaptic reorganization levels (Exp Neurol. 1997 Mar;144(1):174-82. Regeneration of the olfactory tract following neonatal lesion in rats. Munirathinam S et al). This special issue mostly covers the advancement in perception of chemical senses by using PET and fMRI imaging studies, a good read to update Olfactory Sense?.

Our knowledge regarding the neural processing of the three chemical senses has been considerably lagging behind that of our other senses. It is only during the last 25 years that significant advances have been made in our understanding of where in the human brain odors, tastants, and trigeminal stimuli are processed. Here, we provide an overview of the current knowledge of how the human brain processes chemical stimuli based on findings in neuroimaging studies using positron emission tomography and functional magnetic resonance imaging. Additionally, we provide new insights from recent meta-analyses, on the basis of all published neuroimaging studies of the chemical senses, of where the chemical senses converge in the brain.
http://pubs.acs.org/toc/acncdm/2/1
http://pubs.acs.org/toc/acncdm/2/1
Friday, February 25, 2011
Learning EMG control of a robotic hand: towards active prostheses
for those who are interested in "EMG's" and developments in the field of usage of EMGs...!
ABSTRACT
We introduce a method based on support vector machines which can detect opening and closing actions of the human thumb, index finger, and other fingers recorded via surface EMG only. The method is shown to be robust across sessions and can be used independently of the position of the arm. With these stability criteria, the method is ideally suited for the control of active prosthesis with a high number of active degrees of freedom. The method is successfully demonstrated on a robotic four-finger hand, and can be used to grasp objects
Wednesday, January 19, 2011
New Edition Of Aage's Book is Ready in Dec 2010.
From the Back Cover
 The third edition of this classic text again provides practical, comprehensive coverage of the anatomical and physiological basis for intraoperative neurophysiological monitoring. Written by a leading authority in the field, Dr. Aage Moller has updated this important title to again offer all the leading-edge knowledge needed to perform electrophysiological recordings in the operating room, to interpret the results, and to present the results to the surgeon. The field known as "intraoperative monitoring" has expanded rapidly to cover other uses of neurophysiology and electrophysiologic recordings during surgical operations that affect the brain, spinal cord, and other parts of the nervous system. These new areas are covered in this new edition. To better represent the content of the book and the field as it now stands, many of the chapters have been revised and new material has been added. While the general organization of the book is maintained, chapters such as monitoring of motor systems have been revised and extended with new material, including more detailed description of the anatomy and physiology of motor systems and new information about intraoperative monitoring.
The third edition of this classic text again provides practical, comprehensive coverage of the anatomical and physiological basis for intraoperative neurophysiological monitoring. Written by a leading authority in the field, Dr. Aage Moller has updated this important title to again offer all the leading-edge knowledge needed to perform electrophysiological recordings in the operating room, to interpret the results, and to present the results to the surgeon. The field known as "intraoperative monitoring" has expanded rapidly to cover other uses of neurophysiology and electrophysiologic recordings during surgical operations that affect the brain, spinal cord, and other parts of the nervous system. These new areas are covered in this new edition. To better represent the content of the book and the field as it now stands, many of the chapters have been revised and new material has been added. While the general organization of the book is maintained, chapters such as monitoring of motor systems have been revised and extended with new material, including more detailed description of the anatomy and physiology of motor systems and new information about intraoperative monitoring.http://www.amazon.com/Intraoperative-Neurophysiological-Monitoring-Aage-M%C3%B8ller/dp/1441974350/ref=dp_ob_title_bk
Product Details
|
Friday, October 22, 2010
168.4 Billion per Year to treat Obesity?. About 16.5% of America's Medical Spending?.
Obesity is eating up the total medical and health care spending of US, a whopping 16.5% (168.4 Billion) just to treat Obesity alone?. Ref: Cardiovascularbusiness.comUsing instrumental variables (IV) to estimate the impact of obesity on medical costs, researchers found that the causal effect of obesity on medical expenditures is four times higher than when non-IV models are used, indicating that previous literature has underestimated the impact of obesity on medical costs, according to a National Bureau of Economic Research working paper published this month. The report estimates the annual cost of treating obesity-related illnesses annually in the U.S. is $168.4 billion, or 16.5 percent of medical spending. Previous studies have underestimated this cost and reported that obesity is only responsible for 9.1 percent of medical spending.
Sunday, July 18, 2010
Cauda Equina and Conus Medullaris Syndromes
Interesting Read!..
Cauda Equina and Conus Medullaris Syndromes
Introduction
Background
The spinal cord tapers and ends at the level between the first and second lumbar vertebrae in an average adult. The most distal bulbous part of the spinal cord is called the conus medullaris, and its tapering end continues as the filum terminale. The upper border of the conus medullaris is often not well defined. Distal to this end of the spinal cord is a collection of nerve roots, which are horsetail-like in appearance and hence called the cauda equina (Latin for horse's tail). These nerve roots constitute the anatomic connection between the central nervous system (CNS) and the peripheral nervous system (PNS). They are arranged anatomically according to the spinal segments from which they originated and are within the cerebrospinal fluid (CSF) in the subarachnoid space with the dural sac ending at the level of second sacral vertebra.
Thursday, June 24, 2010
Antoun Koht, M.D.
Anesthesiologists should re-evaluate and re-ignite their interest in neurophysiologic monitoring.
Their active involvement could lead to improved neuromonitoring today and allow
for possible supervision in the future.
Currently, neurophysiologic monitoring is conducted by trained technologists capable of
operating the neuromonitoring machine, connecting wires, obtaining reproducible signals,
and identifying signal changes; and they should be able to troubleshoot technical issues contributing to signal changes. However, diagnosis of the etiology of signal changes may be difficult
and outside the realm of their expertise. In order to elucidate signal change etiology, it is necessary to examine all potential causative factors, including rapidly checking monitoring circuit integrity, evaluating patient position, optimizing physiologic status, eliminating pharmacologic contributions, and correlating surgical maneuvers with signal changes.
Saturday, May 29, 2010
ABRET's Policy on ABNM/CNIM Exams: Unfriendly and hindering Prospective Specialists?.
I recently received an email from one of our neuromonitoring colleagues with a serious concern about ABRET's policy on ABNM exams, I hope the ABRET officials read this blog article and also listen to practitioners in the field while drafting policies.
**********************************************************Date: Tue, 25 May 2010 12:08:58 -0700
Subject: need your advice, thanks
From: yingliu.lin@gmail.com
To: edu@drmuni.com
Dear Dr. Muni
My name is pearl, I am a regular reader for your neuromonitoring blog, which really impressed me. I read your article about the critical comment on ABRET's new policy changes on the CNIM requirement, and I am so happy to see the good outcome.
Now I am bothered by ABNM’s new policy changes on applicant’s eligibility. Beginning Aug, 2010, the new policy requires all applicants to provide a statement from a qualifying, supervising neurophysiologist. The new policy defines “a qualifying supervising neurophysiologist is either and individual with board certification from the American board of neurophysiologic monitoring (I think the number of these people is less than 200 in US) ora licensed physician who is board certified in neurology by the American board of psychiatry and neurology and who has fellowship training in clinical neurophysiology including intraoperative neurophysiological monitoring (I don’t know how many people would be qualified for this criteria, even less?), which means if one is not trained by any of these qualifying neurophysiologists, he or she will not get a statement and lose the opportunity to take the exam. Another potential problem is that the exam itself won’t be the major factor to decide whether or not one is competent to be a certificated neurophysiologist because subjective opinions based on personal motives (something like competition) could block a competent person’s opportunity taking the exam. I personally think this is not like a job hunting situation, in which the references recommendation should play the important role in judging a person’s qualification. This is a testing, as long as a candidate meets all of the objective requirements, such as three years experience in the field of neuromonitoring, completing 300 cases, and Ph.D degree in neurophysiology or neuroscience, shouldn’t the exam itself be the first to talk? With the IOM growing so fast, younger qualified people in this field should be encouraged to become board certificated experts, instead of trying to restrict people taking the exam by adding some crap requirements for whatever reasons or purposes. This new change gives a small number of people privilege to determine whether or not one has chance to take the exam even if he or she meets all objective requirements, which undermines the fair competition.
I think you understand my points about this issue, may I know your thoughts, and what is your suggestion if one can not get a statement from a neurophysiologist for the crap reasons?
Thanks for your time; I am looking forward to hearing from you.
All the best
pearl
**************************************************************
This issue was lingering in my mind for quite sometime, when Pearl wrote to me the above e-mail, I realized it is time to make a point on my blog, like Pearl few of my other colleagues who are veterans in this field of neuromonitoring also told me about these policies are rather callous, my friends on the phone expressed their concern about the shrewd and unfriendly policies of ABRET that is going to keep the qualified PhDs away and deprive the neuromonitoring field with only handful of ABNMs?.
ABNM Exams policies are redundant and mundane , further appear to make the candidate miserable with too many useless requirements, in addition to those mundane policies, the exam board seems to fail many candidates, some very talented PhDs and MDs have been failed repeatedly, simply reflecting the motive of ABRET board to make more money out of the candidates in fees?, if this continues, I sincerely hope that ABRET is going to be scrutinized and comes under the radar of US exams regulatory boards. This current article I am writing is mostly to talk about how their policies are framed to make the process of exam cumbersome and ridiculous.Several months ago, ABRET reversed certain policies on CNIM following wide criticism of their CNIM exam requirements , they made it more realistic, appealing and useful to CNIM seekers.
This time, it is about ABNM exams, the number of ABNM certified neurophysiologists/neurologists are very few in US, as of 2008 there were only 128 D-ABNM. And, as per the latest numbers listed on ABNM website, there are only 144 diplomats received the D-ABNM. If the website is not updated in the last two years, it might be another 20-30 candidates in this last two years, adding to be around 175 or 180 diplomats. This is most likely the latest number, this is in all reality is an abysmal count considering the demand and need to have many such highly trained specialists. There is no other country or organization in US or outside to award ABNM, which means that the number quoted above is a global ABNM, there are no such ABNM outside US. And, not even in UK or Canada is there such ABNM diplomats?.Isn't this irony that an organization created to support, promote and safeguard the the field of modern patient care is blocking the prospects of so many PhDs. What is disturbing is the requirements from PhD/MDs to appear for exam, as you will notice in the accompanied E-mail message from Pearl, in order to submit ABNM exam, a highly trained PhD holder with several years of experience in academia or industry, and possibly the PhDs would have had faculty experience, regardless of such high qualification and expertise, like a school student they have to get approval from a board certified Surgeon or a neurophysiologist with a D-ABNM. The application requirement is one of these must sign the application and recommend the candidate, this is ridiculous, ABRETs policy sounds like running kinder garden school, does not look like a advanced medical care providers certification exam.
Why would someone with a PhD and tremendous experience have to stoop to a fellow neurophysiologist with a DBANM or a surgeon to file exam application, why?. Does this make any sense at all??. I can say that my neurophysiology/neuromonitoring CEO or supervisor is a Jerk and stupid, and may be the surgeon I work with do not have expert knowledge in brain and spine, or nervous system. Even neurologists do not have special and advanced knowledge as much as a Neurophysiologist, what a crap is this that a PhD has to go and get his application approved, this policy has to change.ABRET and ABNM must realize that there are shortcomings in the number of D-ABNM, but there are also other issues like the ABNM's can't bill or claim cpt codes like an M.D can do?, this is a terrible policy too!. How many neurologists can set up a neuromonitoring test, prepare the patient, set up protocol, execute an appropriate test, monitor actively, interpret and analyze the data instantly and warn the surgeon about changes?. How many neurologists and spine surgeons and other surgeons really know or have comprehensive knowledge about neurophysiology, the intricacies of evoked potentials?. The clinical training and knowledge is not going to be of much use inside the OR, unless they were trained by a Neurophysiologist as to how to monitor and interpret the signals in the OR.
Hope the ABRET and ASNM look into these and do not bow down to the Medical Association, the neuromonitoring field is developed by decades of hard work and dedication of many neuroscientists and researchers in the field, after decades of establishing this field and make it to applicable in the clinical set up, the medical association and jobless clinicians want to steal away neuromonitoring field with their crap policies and subjugation of the monitoring professionals in the name of medical regulations deliberately designed to keep the MDs running the show?.ABRET has to be thoughtful about their policies besides making PhDs in Neurophysiology and PhDs from related neuroscience fields with D-ABNM should be able to bill like an MD, including the medicare policies where an M.D oversight is currently a requirement, will the ABRET wake up and fight on these issues, as well as keep the exam policies user friendly and approachable for PhDs with experience in neuromonitoring?
This modern and growing health care field needs more doctorate level providers, especially those with PhD in Neurophysiology, or PhDs in allied field with extensive training in Neurophysiology.
Monday, May 17, 2010
American Academy of Neurology-Policy on Intraoperative Neuromonitoring!
The American Academy of Neurology has put up this policy on Intraoperative Neuromonitoring, though old but it is interesting note some observations like the following multicenter evaluation study on SSEPs, it is an impressive result as far as SSEPs concerned.
2. Multicenter Data in Spinal SurgeriesAn extensive multicenter study conducted in 1995 demonstrated that IOM using SEP reduced the
risk of paraplegia by 60% in spinal surgeries (Nuwer et al., 1995). The incidence of false
negative cases, wherein an operative complication occurred without having been detected by the
monitoring procedure, was small: 0.06% (Nuwer et al., 1995).
Friday, April 16, 2010
Pedicle Screws & Triggered EMGs!
Spine (Phila Pa 1976). 2010 Jan 15;35(2):E43-8.
STUDY DESIGN: This is a retrospective analysis of 30 pediatric deformity surgeries. OBJECTIVE: The purpose of this study was to evaluate the accuracy of neuromonitoring in comparison to postoperative computed tomography scans for pedicle screw position. SUMMARY OF BACKGROUND DATA: Triggered electromyography potentials in aiding the placement of lumbar pedicle screws are considered useful; however, this method is less accepted in thoracic screw placement. METHODS: Thirty pediatric deformity surgeries were reviewed. All screws were placed using fluoroscopic assistance. Electromyography data were obtained on all screws. Every patient underwent postoperative computed tomography scanning. Computed tomography scans were assessed by all authors, and each screw was classified. Sensitivity, specificity, negative predictive value, and likelihood ratios were determined for the cut-off value of an electromyography > or =6 mA. RESULTS: A total of 329 screws were reviewed. No complications occurred. An overall accuracy of 93% was obtained. No retained screw had greater than 2 mm medial pedicle wall breach. Nine screws were removed intraoperatively due to medial breach. The mean electromyography potential for all classes of screws was not statistically different (P > 0.1). The negative predictive value of the test was 0.92 in the thoracic spine and 0.93 in the lumbar spine. The negative likelihood ratios were 0.96 and 0.35 for the thoracic and lumbar spines respectively, and the positive likelihood ratio was 1.4 for the thoracic spine and 12.5 for the lumbar spine. CONCLUSION: Thoracic and lumbar pedicle screws are safe surgical options in the treatment of pediatric scoliosis. Comparison of electromyography potentials and postoperative computed tomography scans showed no statistically significant difference for all classes of screws. The likelihood ratio for electromyography testing was more clinically significant in the lumbar spine. A triggered electromyography value greater than or equal to 6 mA has a high likelihood of that screw being in the "safe zone." However, there is no true electromyography cut-off value that guarantees accurate placement and avoidance of neurologic injury.
Usefulness of electromyography compared to computed tomography scans in pedicle screw placement.Duffy MF, Phillips JH, Knapp DR, Herrera-Soto JA.
STUDY DESIGN: This is a retrospective analysis of 30 pediatric deformity surgeries. OBJECTIVE: The purpose of this study was to evaluate the accuracy of neuromonitoring in comparison to postoperative computed tomography scans for pedicle screw position. SUMMARY OF BACKGROUND DATA: Triggered electromyography potentials in aiding the placement of lumbar pedicle screws are considered useful; however, this method is less accepted in thoracic screw placement. METHODS: Thirty pediatric deformity surgeries were reviewed. All screws were placed using fluoroscopic assistance. Electromyography data were obtained on all screws. Every patient underwent postoperative computed tomography scanning. Computed tomography scans were assessed by all authors, and each screw was classified. Sensitivity, specificity, negative predictive value, and likelihood ratios were determined for the cut-off value of an electromyography > or =6 mA. RESULTS: A total of 329 screws were reviewed. No complications occurred. An overall accuracy of 93% was obtained. No retained screw had greater than 2 mm medial pedicle wall breach. Nine screws were removed intraoperatively due to medial breach. The mean electromyography potential for all classes of screws was not statistically different (P > 0.1). The negative predictive value of the test was 0.92 in the thoracic spine and 0.93 in the lumbar spine. The negative likelihood ratios were 0.96 and 0.35 for the thoracic and lumbar spines respectively, and the positive likelihood ratio was 1.4 for the thoracic spine and 12.5 for the lumbar spine. CONCLUSION: Thoracic and lumbar pedicle screws are safe surgical options in the treatment of pediatric scoliosis. Comparison of electromyography potentials and postoperative computed tomography scans showed no statistically significant difference for all classes of screws. The likelihood ratio for electromyography testing was more clinically significant in the lumbar spine. A triggered electromyography value greater than or equal to 6 mA has a high likelihood of that screw being in the "safe zone." However, there is no true electromyography cut-off value that guarantees accurate placement and avoidance of neurologic injury.
New Guidlines for TCD!
J Neuroimaging. 2010 Mar 17. [Epub ahead of print]
American Society of Neurophysiologic Monitoring and American Society of Neuroimaging Joint Guidelines for Transcranial Doppler Ultrasonic Monitoring.
Edmonds HL Jr, Isley MR, Sloan TB, Alexandrov AV, Razumovsky AY.
The American Society of Neurophysiologic Monitoring (ASNM) and American Society of Neuroimaging (ASN) Guidelines Committees formed a joint task force and developed guidelines to assist in the use of transcranial Doppler (TCD) monitoring in the surgical and intensive care settings. Specifically, these guidelines: (1) delineate the objectives of TCD monitoring; (2) characterize the responsibilities and behaviors of the sonographer during monitoring; (3) describe methodological and ethical issues uniquely relevant to monitoring. The ASNM and ASN strongly support the positions that (1) acquisition and interpretation of intraoperative TCD ultrasonograms be performed by qualified individuals, (2) service providers define their diagnostic criteria and develop on-going self-validation programs of these performance criteria in their practices. We agree with the guidelines of other professional societies regarding the technical and professional qualifications of individuals responsible for TCD signal acquisition and interpretation (Class III evidence, Type C recommendation). On the basis of current clinical literature and scientific evidence, TCD monitoring is an established monitoring modality for the: (1) assessment of cerebral vasomotor reactivity and autoregulation; (2) documentation of the circle of Willis functional status; (3) identification of cerebral hypo- and hyperperfusion, recanalization and re-occlusion; and (4) detection of cerebral emboli (Class II and III evidence, Type B recommendation). J Neuroimaging 2010;XX:1-7.
American Society of Neurophysiologic Monitoring and American Society of Neuroimaging Joint Guidelines for Transcranial Doppler Ultrasonic Monitoring.
Edmonds HL Jr, Isley MR, Sloan TB, Alexandrov AV, Razumovsky AY.
The American Society of Neurophysiologic Monitoring (ASNM) and American Society of Neuroimaging (ASN) Guidelines Committees formed a joint task force and developed guidelines to assist in the use of transcranial Doppler (TCD) monitoring in the surgical and intensive care settings. Specifically, these guidelines: (1) delineate the objectives of TCD monitoring; (2) characterize the responsibilities and behaviors of the sonographer during monitoring; (3) describe methodological and ethical issues uniquely relevant to monitoring. The ASNM and ASN strongly support the positions that (1) acquisition and interpretation of intraoperative TCD ultrasonograms be performed by qualified individuals, (2) service providers define their diagnostic criteria and develop on-going self-validation programs of these performance criteria in their practices. We agree with the guidelines of other professional societies regarding the technical and professional qualifications of individuals responsible for TCD signal acquisition and interpretation (Class III evidence, Type C recommendation). On the basis of current clinical literature and scientific evidence, TCD monitoring is an established monitoring modality for the: (1) assessment of cerebral vasomotor reactivity and autoregulation; (2) documentation of the circle of Willis functional status; (3) identification of cerebral hypo- and hyperperfusion, recanalization and re-occlusion; and (4) detection of cerebral emboli (Class II and III evidence, Type B recommendation). J Neuroimaging 2010;XX:1-7.
Thursday, March 18, 2010
How Do You Come Across to Patients?
Health Care providers service organization (HFSO) has this advice for you, yes they are right.
How Do You Come Across to Patients?
What patients think of you is just as important as the quality of the care you provide. Patients’ perception of your interest and compassion determines how satisfied they are with the care they receive. And satisfied patients are less likely to sue.
To make sure patients see you in the best possible light, be friendly, but respectful. Don’t call your patient by his first name, for example, unless he asks you to. If you’re a physical therapist, athletic trainer, massage therapist, or other healthcare professional where therapeutic touch is crucial, you’ll want to avoid being overly friendly.
You don’t want patients to misconstrue therapeutic touch as personal. If patients do share something of a personal nature with you— such as the fact that they’re going through a divorce—bring it back to the matter at hand: their health. Ask how the stress might be affecting their response to therapy.
Being professional, however, doesn’t mean that you need to appear rude, condescending, or disinterested. Despite the pressures of managed care, don’t rush patients through their visit. Listen to their questions and concerns attentively: Something seemingly trivial may be important to them and may even clue you into an important aspect of their care.
Remember that some patients, particularly those who don’t feel well, have trouble processing information in times of stress. They won’t hear what you say if they feel intimidated, or get the sense that you’re not addressing their concerns. Your friendly and professional demeanor will help them relax, meaning that they’ll be more likely to understand your instructions and less likely to blame you if something goes wrong with their care.
Saturday, February 27, 2010
Society for Neuroscience & News!
 SFN is fighting for better funding and support for Neuroscience and allied research fields. Join hands with sfn, it is for a good cause. Bush govt destroyed the academic and research atmosphere in US cutting budget and shrinking the funds to overall research, I hope with President Obama in office, our hope is that he understands scientific research is the backbone of a nation's growth and prosperity.
SFN is fighting for better funding and support for Neuroscience and allied research fields. Join hands with sfn, it is for a good cause. Bush govt destroyed the academic and research atmosphere in US cutting budget and shrinking the funds to overall research, I hope with President Obama in office, our hope is that he understands scientific research is the backbone of a nation's growth and prosperity.News
Attend SfN Capitol Hill Day to Build Support for Research; More Recovery Act Stories Needed
Join your colleagues in Washington for the 2010 SfN Capitol Hill Day on March 25 to meet your legislators in person and share the story of your research and its health and economic benefits. Your voice is needed to support the scientific community's request of $35 billion for NIH and $7.4 billion for NSF in FY2011. Also key to this year's advocacy efforts are the new "In the Lab: Recovery Act Stories", which illustrate how Recovery Act-funded research is improving health, while contributing to the economy. Visit the SfN Recovery Act page for additional resources and to log-in and submit your own story today! Contact advocacy@sfn.org with questions.

Clinical Neurophysiology, a facelift to EEG & EP journals!
As of January 1999, The journal Electroencephalography and Clinical Neurophysiology, and its two sections Electromyography and Motor Control and Evoked  Potentials have amalgamated to become this journal - Clinical Neurophysiology Clinical Neurophysiology is the official journal of the International Federation of Clinical Neurophysiology, Italian Clinical ...
Potentials have amalgamated to become this journal - Clinical Neurophysiology Clinical Neurophysiology is the official journal of the International Federation of Clinical Neurophysiology, Italian Clinical ...
click here for full Aims & Scope
As of January 1999, The journal Electroencephalography and Clinical Neurophysiology, and its two sections Electromyography and Motor Control and Evoked Potentials have amalgamated to become this journal - Clinical Neurophysiology
Potentials have amalgamated to become this journal - Clinical Neurophysiology Clinical Neurophysiology is the official journal of the International Federation of Clinical Neurophysiology, Italian Clinical ...click here for full Aims & Scope
Clinical Neurophysiology is the official journal of the International
Federation of Clinical Neurophysiology, Italian Clinical Neurophysiology
Society, The Japanese Society
of Clinical Neurophysiology. It is dedicated to fostering research and
disseminating information on all aspects of Clinical Neurophysiology, both
normal and abnormal. The journal aims at publishing scholarly reports on human
physiology and pathophysiology of both the central and the peripheral nervous
system. The journal is interested in manuscripts reporting data on integrated
neuroimaging of central nervous functions including, but not limited to,
functional MRI, MEG, EEG, PET and other aspects of neuroimaging.
Electromyography, motor control and somatosensory physiopathology are covered by
the journal, as well as evoked potentials with special emphasis on studies of
cognitive functions. Studies on animals and technical notes must have clear
relevance and applicability to humans.
Intraoperative Neurophysiological Monitoring, by Leon K Liem
eMedicine
Liem's article on "Intraoperative Neurophysiological
monitoring", a good place for starters to know the basics of
neuromonitoring. Author: Leon K Liem, MD, Assistant Clinical Professor, Division of Neurological Surgery, University of Hawaii, John Burns School of Medicine
Liem's article on "Intraoperative Neurophysiological
monitoring", a good place for starters to know the basics of
neuromonitoring. Author: Leon K Liem, MD, Assistant Clinical Professor, Division of Neurological Surgery, University of Hawaii, John Burns School of Medicine
Contributor Information and Disclosures
Updated: Feb 11, 2010
Introduction
This article provides an overview of the various neurophysiological monitoring techniques used intraoperatively.
Intraoperative neurophysiological monitoring has been utilized in attempts to minimize neurological morbidity from operative manipulations. The goal of such monitoring is to identify changes in brain, spinal cord, and peripheral nerve function prior to irreversible damage. Intraoperative monitoring also has been effective in localizing anatomical structures, including peripheral nerves and sensorimotor cortex, which helps guide the surgeon during dissection.
Evoked potential monitoring includes somatosensory evoked potentials (SSEP), brainstem auditory evoked potentials (BAEP), motor evoked potentials (MEP), and visual evoked potentials (VEP). Electromyography (EMG) also is used extensively during operative cases. Scalp electroencephalography (EEG) provides data for analysis in SSEP, BAEP, and VEP. Scalp EEG also can be used to monitor cerebral function during carotid or other vascular surgery. In addition, EEG recorded directly from the pial surface, or electrocorticography (ECoG), is used to help determine resection margins for epilepsy surgery, and to monitor for seizures during electrical stimulation of the brain carried out while mapping cortical function. http://emedicine.medscape.com/article/1137763-overview
ABNM- Latest Schedules of Exams
 |
Neurophysiologic Monitoring |
Next Written Exams
Next Oral Exams
For information about registering for these tests | ||||||||||||||||||||
Subscribe to:
Posts (Atom)